
No products in the cart.
Information About Glaucoma
Overview
Often known as the “sneak criminal of sight,” eye disease refers to a bunch of eye diseases that harm the nerves carrying pictures from the attention to the brain. Primary open angle glaucoma (POAG) is a leading cause of blindness in the United States, according to the National Eye Institute. A study revealed within the journal Archives of medical specialty estimates that two.2 million Americans have the unwellness, but half don’t know it. Glaucoma usually produces no symptoms until the disease has progressed to the point of damaging a person’s sight.
Although glaucoma has no cure, it can be controlled and vision can be maintained if it is detected early. That’s why comprehensive eye examinations are recommended at least every two years after age 35 for those at increased risk for the disease. Although anyone will get eye disease, the danger is higher for those over age sixty, those who have a family history of the condition and African Americans. Older Hispanics/Latinos are also at elevated risk, the highest prevalence being among those of Mexican descent.
Other risk factors include:
- diabetes
- nearsightedness, called myopia
- regular, long-term corticosteroid use, particularly if in the form of eyedrops
- previous eye injury
Another risk issue for eye disease is high at intervals the attention. Pressure in the eye is known as intraocular pressure. However, it’s a standard idea that having high force per unit area suggests that you’ve got eye disease. In fact, you’ll have high force per unit area, known as ocular hypertension, and not have glaucoma. Whether you develop glaucoma depends on how much pressure your optic nerve—the bundle of 1.2 million nerve fibers that transmits images from the eye to the brain—can take without being damaged.
The first step in understanding eye disease and its relationship to force per unit area is learning however the attention works. The outer protecting layer of eye includes clear tissue through that light-weight enters, known as the cornea. The iris is the colored part of the eye containing muscles that make the pupil open and close. The pupil is the black area in the center of the eye where light enters. Located inside the eye, behind the iris, is the lens. The lens is a transparent structure with an outward curve on both sides that focuses light onto the retina at the back of the eye. The membrane is created of sensitive tissue that sends visual messages via nerve impulses to the brain through the nervus opticus. The brain then processes the optic nerve’s signals into the images that you see.
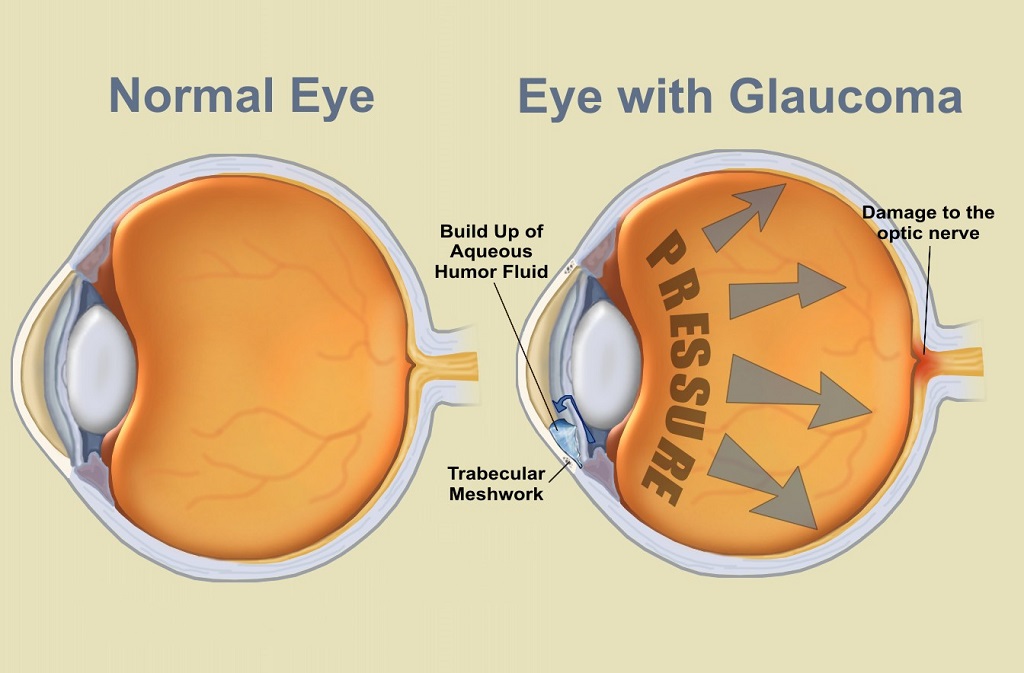
The anterior chamber may be a house within the eye boxed by the membrane, iris, pupil and lens. Flowing through this chamber may be a liquid, called the aqueous humor, which supplies oxygen and nutrients to the cornea and lens and helps maintain the shape of the eyeball. A tiny gland, called the ciliary body, is located behind the iris and produces the fluid. The fluid travels from the secreter through the pupil into the anterior chamber, exiting at Associate in Nursing angle wherever the membrane and also the iris meet. At the angle is a spongy mesh of tissue that works like a drain, called the trabecular meshwork.
There are several forms of glaucoma, including the following:
- Open-angle. during this most typical type of eye disease, the angle wherever the membrane and therefore the iris meet is open, however the body fluid fluid passes too slowly through the mesh drain. As a result, the pressure within the eye step by step will increase. This compresses cells in the optic nerve. If left untreated, the compression eventually kills the cranial nerve cells, inflicting sightlessness.Early detection is essential to managing open-angle glaucoma and minimizing vision loss. Treatments include medications in the form of eyedrops and pills to reduce the amount of fluid (aqueous humor) in the eye or improve its drainage. Both treatments help reduce intraocular pressure. Surgery, by optical maser or standard means that, conjointly could also be suggested.
- Normal-tension. Some folks with traditional eye pressure develop eye disease, a sickness called low-tension or normal-tension eye disease (NTG). In this form of the disease, eye pressures are within the normal range, but the optic nerve progressively deteriorates. The progression of the disease is faster in those who have the specific risk factors for progression, namely, Japanese ancestry,cardiovascular disease, family history of any kind of glaucoma and being female. Research is continuous on this manner of eye disease, that is believed to be associated with poor blood flow to the cranial nerve.
- Pigment dispersion syndrome affects young myopic individuals. Glaucoma occurs when grains of pigment from the back of the iris flake off into the aqueous humor, eventually clogging the drainage meshwork and raising eye pressure. The syndrome produces no noticeable symptoms however are often detected and monitored in routine eye examinations. According to the yankee Academy of medical specialty, concerning thirty % of individuals with pigment dispersion syndrome develop pigmentary eye disease, a type of open-angle glaucoma. In this kind of eye disease, travail will cause a pigment shower and cause muzzy vision from the inflated pressure.
- Angle-closure. Angle-closure. acute glaucoma happens in 2 forms: acute and chronic. The acute kind can be a sudden, painful attack requiring emergency treatment. The chronic version happens over time, producing no recognizable symptoms before vision is lost.Risk factors include:
- Hyperopia
- Being of Asian decent
People with acute glaucoma tend to own a smaller-than-average anterior chamber, and the angle between the iris and the cornea where the aqueous humor drains is also smaller. When the lens naturally grows larger with advancing age, the aqueous humor has difficulty flowing in the tight space, causing the fluid to build up behind the iris, narrowing the angle even more. When the pupil dilates, such as when entering a dark room, or when experiencing anxiety or stress, taking certain over the counter medications or medications with the glaucoma warning label, the angle can narrower even further, and the iris is forced against the trabecular meshwork, stopping drainage. Without drainage, pressure in the eye squeezes and damages the optic nerve.
In acute acute glaucoma, pressure rises suddenly, manufacturing pain. The eye turns red, the cornea swells and clouds, vision may be blurred and lights may appear as if they have halos. Acute angle-closure glaucoma is a medical emergency. To treat it, health care professionals may initially administer medications to reduce eye pressure as fast as possible until a surgery callediridotomy can be done. Iridotomy is a procedure that uses a laser to make a tiny hole in the iris to improve the flow of the aqueous humor.
In chronic glaucoma, the iris step by step closes over the drain, inflicting no recognizable symptoms. As this happens, scars type between the iris and therefore the drain, eventually obstruction it and driving up force per unit area. Treatment may include eyedrops and surgery
- Pseudoexfoliation glaucoma Pseudoexfoliation eye disease happens once a whitish material, usually found on all surfaces of the attention, causes preventative of the eye’s emptying material and will increase the force per unit area. While pseudoexfoliation eye disease causes no noticeable symptoms, it can be detected through a routine exam. Many people with pseudoexfoliation eye disease area unit of European descent. Over time, the at first open angle might slim and shut because the lens within the eye will increase in size with age. It can lead to angle closure glaucoma. This type of glaucoma is secondary; the whitish pseudoexfoliation material causes the problem
Diagnosis
No single test is 100 percent effective in determining whether you have glaucoma. To diagnose the disease, your health care professional will ask you questions about your medical history. You should receive a comprehensive eye examination, which may include any of the following painless tests:
- Visual acuity. This test measures the ability of your central vision to distinguish details and shapes. You will be asked to cover an eye and read a chart to measure how well you see at various distances.
- Tonometry. This is a test to measure your intraocular pressure. It can be performed in a variety of ways. In Goldman applanation tonometry, you are given drops to numb your eye, and a pressure-sensitive tip is placed against the eye to measure its pressure. This method is the most accurate way of measuring pressure but is limited when there is an irregularity of the corneal surface. A tono-pen is a handheld instrument that is portable and can measure pressure when the device is placed against the eye. No instrument touches the eye in noncontact, or “air puff” tonometry, in which air is blown at the eye and pressure assessed by the eye’s resistance to it.
- Gonioscopy. In this test, a special lens containing a mirror is placed lightly on the front of your eye. It allows the health care professional to examine the angle between the cornea and the iris inside the eye.
- Pachymetry. This test uses a measuring device to determine the thickness of your corneas. Central corneal thickness (CCT) is an important factor in diagnosing glaucoma. Thick corneas may increase eye-pressure readings in people who do not have glaucoma. However, individuals with skinny corneas might have traditional pressure readings however still have eye disease. A thick CCT leads to an overestimation of the pressure, while a thin CCT leads to an underestimation of the pressure. The health care professional takes central corneal thickness into consideration when assessing risk factors.
- Perimetry. This test, also called a visual field test, measures your side or peripheral vision. Today it is often done with computerized equipment. You place your chin on a stand in front of a computerized screen. You are asked to focus on a spot on the screen and push a button or indicate when you see a tiny flash of light. This gives your health care professional a “map” of your field of vision.
- Ophthalmoscopy.In this test, your health care professional places drops in your eyes to widen, or dilate, your pupils. Then the health care provider appearance through the pupil at the cranial nerve employing a special instrument (ophthalmoscope) or with special lens that magnifies details at the rear of the attention. Your close vision may be blurred for several hours after this examination until the dilating drops wear off.
Treatment
Glaucoma treatments generally focus on reducing intraocular pressure to a level the health care professional believes will not cause further damage to the optic nerve. This level is often called the “target pressure,” and it differs from person to person and may change over the course of treatment. Eye pressure is measured in millimeters of mercury (mm Hg). It varies, even throughout a single day. Generally, eye pressure readings between 10 and 21 mm Hg are considered normal, although a person may have glaucoma even with pressures in this range.
Most new diagnosed cases of eye disease area unit treated with medications, that are available in topical and oral type. Topical medications may be eyedrops or eye ointments. Oral eye disease medications are available in pill and pill type.
The most common topical medications are eyedrops, and some of them must be taken once or several times a day. Most topical medications cut back eye pressure by either increasing the flow of the bodily fluid out of the attention or reducing the number of the fluid created within the eye. The following are types of topical glaucoma medications:
- Prostaglandin analogsThis class of drugs works near the drainage area of the eye to stimulate outflow of fluid (aqueous humor) through pathways in the eye other than through the trabecular meshwork. Latanoprost (Xalatan), travoprost (Travatan Z) and bimatoprost (Lumigan) are medications in this class used for glaucoma and hypertension of the eye. Typical dosage is one drop, once a day in the evening. Although this drug tends to be tolerated, it’s some uncommon facet effects. The iris may turn browner in hazel colored eyes after use over several months. Eyelid skin color also may darken.Eyelashes may become longer, thicker and darker. These changes occur solely within the eye receiving the drops and should be permanent. Other possible side effects that may or may not persist include eye burning, itching, stinging, orbital atrophy, dryness of the eye and the feeling that something is in the eye.Prostaglandins may worsen other eye diseases such as iritis or uveitis. This class of medications is avoided in eyes that are at risk for a buildup of fluid in a part of the retina that allows the sight of fine details (called macular edema). Notify your health care skilled if you have got urinary organ or liver diseases, as these drugs’ side effects may increase from higher concentrations remaining in your system.Like other kinds of glaucoma eye drops, the prostaglandin analogs may make the eye more sensitive to light if the individual has uveitis or iritis (inflammation of the eye).
- Carbonic anhydrase inhibitors. For many years these medication were solely out there in pill type however area unit currently out there as eye drops. They cut back the number of bodily fluid the attention produces. Brinzolamide (Azopt) and dorzolamide (Trusopt) area unit used for eye disease and ocular high blood pressure. A combination of Trusopt and Timoptic, called Cosopt, is commonly used. These are generally taken as one drop, two to three times a day. If you have severe kidney disease or liver diseases, talk to your health care professional before taking these drugs as their side effects can increase because of slower removal from your system.Common side effects that may disappear over time include: temporary blurred vision after application and a bitter, sour or unusual taste in the mouth. Less common area unit burning or stinging of the attention upon application, dry eye and strange weariness. Also possible are gastrointestinal symptoms or a runny nose.
- Alpha-adrenergic agonists. These drops also reduce the amount of aqueous humor the eye produces and are used to treat glaucoma and hypertension of the eye. They are chemically related to drugs used to treat high blood pressure. Apraclonidine (Iopidine) is employed most frequently in a very higher concentration before and once some styles of eye disease optical maser surgery to stop or management an increase in eye pressure that is common after the procedure. A combination of Brimonidine and Timoptic, called Combigan, is commonly used.Brimonidine is most commonly used in this class of medication twice to three times a day. Side effects that may or may not persist with both drugs include allergic conjunctivitis, dizziness, dryness of mouth, eye discomfort and fatigue. Before taking brimonidine, tell your health care professional if you have heart or blood vessel diseases, low blood pressure, kidney or liver disease or depression. The drug can increase blood pressure and aggravate depression. Side effects of the drug may increase if you have kidney or liver disease. Additionally, brimonidine should not be taken while taking, or within two weeks of taking, certain kinds of antidepressant drugs called monoamine oxidase (MAO) inhibitors.
- Miotics. These medication increase the speed at that the liquid body substance flows out of the attention. Pilocarpine is that the oldest reflex wont to treat eye disease. It comes in drop and ointment form. Dosage for the drops is usually one drop, fourfold daily. It is not used as often since the newer medications have fewer side effects.Pilocarpine usually contracts the pupil, which lets less light into the eye, resulting in darkened or dim vision and reduced night vision. Blurred vision also may occur for several hours after taking the drug. Eye irritation and headache might occur, however these area unit less common aspect effects and should disappear over time.Carbachol is another miotic that is prescribed in drop form. It helps to open the attention’s drain and increase the speed of fluid flowing out of the eye. It is rarely used, but effective.The most important thing to remember when taking glaucoma medications is to take them as directed by your health care professional. For the medication to figure effectively, they have to be taken frequently and while not interruption. If you have multiple drops, remember to wait a minimum of five minutes between drops or close your eyes for three minutes. You will need to take them as long as they control your eye pressure. If you forget to take your medication, restart them right away.
Surgery
If medications fail to lower your eye pressure, your health care skilled might advocate surgery, either by laser or by conventional operative techniques. Sometimes surgery is recommended as the first-line treatment.
Laser surgery uses a focused beam of sunshine to open clogged evacuation canals. Most laser surgeries can be done on an outpatient basis. First the eye is numbed with drops that last throughout the procedure. Then a health care professional holds a special lens to the eye, and the laser beam is aimed at the lens and reflected onto its target. The person sees a bright light, similar to a camera flash, and usually feels little or no discomfort. After treatment, the eye may be irritated and vision may be blurred. Drops for soreness may be prescribed. Normal activities usually can be resumed after the procedure. Follow-up visits with your health care professional will be required to monitor intraocular pressure.
The following are types of laser surgeries:
- Trabeculoplasty. For people with open-angle glaucoma, a laser is used to open the trabecular meshwork drainage area in the eye, which allows the aqueous humor fluid to move more freely and reduces intraocular pressure. In this procedure, the laser makes tiny burns in the meshwork, which stretches and opens the drainage holes. Intraocular pressure is checked after the procedure, and usually drops are given to be used at home for soreness or swelling inside the eye. In some cases, only half of the meshwork may be treated in one surgery. The remainder is treated in an exceedingly later optical device surgical session. If you have got eye disease in each eyes, only one eye will be treated at a time. The multisession approach allows the physician to decide if additional sessions are needed to reach the target pressure.Research shows that laser trabeculoplasty is very good at lowering intraocular pressure in some people. However, its effects can wear off over time. Your doctor may suggest further treatment. Another sort of trabeculoplasty, called selective laser trabeculoplasty, has been introduced. It treats specific pigmented cells “selectively” and leaves the untreated parts of the fibrous tissue fabric intact. For this reason, SLT may be repeated several times and may also be an option for people with glaucoma who have not had success with traditional laser surgery or pressure-lowering drops.
- Iridotomy. For folks with glaucoma, this surgery uses the laser beam to make a tiny hole in the iris to improve the flow of the aqueous humor to the drainage meshwork.
- Cyclophotocoagulation. Used most often in advanced or severe cases of glaucoma, this procedure uses the laser beam to destroy parts of the ciliary body that produce the aqueous humor fluid. With less fluid flowing through the eye, the intraocular pressure is reduced. A local anesthetic is used to numb the eye.Conventional, incisional surgery often is recommended after medications and laser surgery have failed to control intraocular pressure. The surgery, called filtering microsurgery, creates a new opening for the intraocular fluid to leave the eye. It is performed in a hospital or clinic under local anesthesia and sometimes with sedation.The procedure involves creating a small hole to bypass the normal drainage channel through which the aqueous humor can flow. The sclera is covered by a thin clear layer of tissue called the conjunctiva. When the channel is created, the aqueous humor flows through it and under the conjunctiva, reducing pressure in the eye. Conventional surgery is 60 percent to 80 percent effective at lowering intraocular pressure.After the procedure, eyedrops are used to ward off infection and swelling. Pain medications also may be given for any postoperative discomfort. A patch may be placed over the eye to protect it for 24 hours. A protect is also used for many weeks to still shield the attention from trauma. Recovery takes about six weeks. Weekly follow-up visits with the health care professional will be required for the first few weeks after surgery to check eye pressure and functioning of the new channel. In some cases, a tiny metallic implant (express shunt) is placed in the eye to help lower pressure. Other surgical techniques currently area unit being tired the angle like the trabectome.Like any form of surgery, both laser and conventional surgeries for glaucoma do carry risks. Although unusual, the complications that can occur include:
- infection
- bleeding
- swelling of blood vessels behind the eye
- undesirable changes in intraocular pressure
- loss of vision
- development of cataracts
Another approach to filtering surgery is that the use of evacuation devices like Ahmed eye disease shunt, Krupin valve, Molteno implant and Baerveldt implant. Their use has increased in recent years.
Prevention
Vision loss from glaucoma can be prevented if the disease is detected and treated in time. Because glaucoma rarely produces symptoms until it has progressed, regular eye examinations are the key to early detection and treatment. For those with no risk factors, the American Academy of Ophthalmology recommends a complete eye exam once in your 20s and twice in your 30s. You should have a baseline comprehensive eye exam at age 40, and your eye doctor will recommend follow-up exams based on your family history and the results of the baseline exam. After age 65, it’s important to have a complete eye exam every year or two.
You’re at risk of developing glaucoma if you are older than age 60; are African American, an older Latino, especially of Mexican descent; have a family member who has glaucoma; are very nearsighted; are diabetic; have had an eye injury in the past; or have been taking steroid or cortisone medications regularly. In such cases, you should have an eye exam including tests for glaucoma every one to two years after age 35.
If you are African American, your risk of developing the open-angle type of glaucoma is higher than for Caucasian people, according to the National Eye Institute. Open-angle glaucoma accounts for 19 percent of all blindness among African-Americans, compared to only 6 percent in Caucasians. Older Hispanics/Latinos are also at elevated risk, with the highest prevalence for glaucoma being among those of Mexican descent. Individuals who are far-sighted (hyperopic), with narrow angles and of Asian descent are at risk for acute or chronic angle glaucoma.
Although there’s no best-known thanks to forestall eye disease, maintaining a healthy lifestyle may help you generally avoid diseases. Eating a balanced diet is the best way to ensure your body receives the proper nutrients it needs to function. Some of the vitamins and minerals that contribute to overall eye health embody inhibitor vitamins A, C and E, and minerals zinc, copper and selenium. If you’re concerned about your diet, talk with your health care professional about whether you should take nutritional supplements or make dietary changes.
Getting regular exercise also is a component of maintaining good overall health, and there is some evidence in the medical literature that regular aerobic exercise may help reduce eye pressure. In fact, some studies indicate that exercise that raises the pulse rate by just 20 percent to 25 percent (for example, a brisk walk) for 20 minutes, at least four times a week, can help reduce intraocular pressure, according to the Glaucoma Foundation. Before starting any exercise program, make sure you discuss possible effects on your intraocular pressure with your health care professional. Some forms of glaucoma, such as angle-closure, are unresponsive to exercise or run the risk of increasing eye pressure. Additionally, exercises or yoga movements that hold the head upside down have the potential for increasing eye pressure and generally are discouraged for everyone with glaucoma.
If you are diagnosed with glaucoma, it doesn’t mean you will become blind. To control your disease and protect the sight you have, adhere to the prescription drug regimen recommended by your health care professional and have regular eye examinations to monitor the disease
Facts to Know
- Glaucoma is a group of eye diseases that, when left untreated, damage the optic nerve and can lead to blindness.
- Often called the “sneak thief of sight,” glaucoma usually produces no early warning signs and no symptoms until it has progressed to the point of stealing sight.
- More than 2.2 million Americans have glaucoma, but half don’t know it, according to the National Eye Institute.
- The risk of sightlessness from eye disease is fourfold larger in African Americans than in Caucasians overall, and 14 to 17 times greater in African Americans age 45 to 65 than in Caucasians of the same age, according to Prevent Blindness America
- You are at risk for developing glaucoma if you are African American, are over age 60, have family members with glaucoma, are diabetic or are very nearsighted.
- Open-angle glaucoma is the most common form of glaucoma.
- Glaucoma can occur in children as well as adults. About one out of every 10,000 babies in the United States is born with glaucoma.
- Glaucoma has no cure, but it can be controlled. Treatment may include medications and surgery.
- Although treatment for glaucoma focuses on reducing pressure in the eye, it is possible to have higher than normal eye pressure and not have glaucoma.
- There is no way to prevent glaucoma, but getting regular, comprehensive eye examinations is the best way to identify disease before it affects vision.
Key Q&A
- Does glaucoma always lead to blindness?No. Although glaucoma is a leading cause of blindness in the United States, it can be controlled and vision maintained if it is detected early. Because the disease usually produces no symptoms until it has begun to damage a person’s sight, many of those who have it don’t know it. That’s why comprehensive eye examinations are recommended at least every two years starting at age 35 for those at increased risk for the disease.
- What are the risk factors for glaucoma?You are at risk of developing glaucoma if you are older than age 60, African American, Latino (especially of Mexican descent), have a family member who has glaucoma, are very nearsighted, are diabetic, have had an eye injury in the past or have been taking steroid or cortisone medications for a length of time. In such cases, you should have an eye exam including tests for glaucoma every one to two years after age 35. If you’re African yankee, your risk is especially great. The National Eye Institute reports that African Americans are six to eight times more likely than Caucasians to develop glaucoma.
- What’s the difference between high eye pressure and glaucomaGlaucoma is a group of eye diseases that damages the nerves carrying images from the eye to the brain. When the fluid inside the eye that nourishes the cornea and the lens can’t flow properly through the eye, pressure in the eye builds. The pressure compresses the optic nerve and can damage it. Whether you develop glaucoma depends on how much pressure your optic nerve can take without being damaged.
- My eye pressure is 22 mm Hg. Does that mean I have glaucoma?Not necessarily. Eye pressure is measured in millimeters of mercury (mm Hg), and it varies, even throughout the day. Generally, eye pressure readings between 10 and 20 mm Hg are considered normal, although a person may have glaucoma even with pressures in this range. It’s a common thought that having high force per unit area means that you’ve got eye disease. In fact, you’ll be able to have high force per unit area, known as ocular hypertension, and not have glaucoma. In some individuals, the second cranial nerve will tolerate pressures on top of the vary thought-about traditional. The only way to determine whether you have glaucoma is to have a comprehensive eye examination.
- What is the most common type of glaucoma?Open-angle glaucoma is that the commonest type of the illness. In glaucoma, the angle wherever the tissue layer and also the iris meet within the eye is open, however the body fluid fluid passes too slowly through the meshing drain. As a result, the pressure within the eye step by step will increase, compressing cells in the optic nerve. If left untreated, the compression eventually can cause the nervus opticus cells to die, producing blindness.
- What is the most common treatment for glaucoma?Glaucoma is most commonly treated with prescription medications in the form of eyedrops. Many of the prescriptions must be taken once to several times a day. Glaucoma medications, which may are available topical or oral type, are designed to lower pressure in the eye. Other glaucoma medications come in the form of a gel. Most topical medications scale back eye pressure by either increasing the flow of the body fluid fluid out of the attention or reducing the number of the fluid created within the eye. Oral eye disease medications are available pill and pill type and area unit aimed toward speed production of fluid within the eye.
- Can surgery help my open-angle glaucoma?Possibly. If medications fail to lower your eye pressure, your health care professional may recommend surgery, either by laser or by conventional operative techniques. Sometimes surgery is recommended as the first-line treatment. In a procedure called laser trabeculoplasty, a beam of concentrated light is used to open the drainage area in the eye. This allows the fluid in the eye to move more freely and reduces intraocular pressure. The effects of optical device treatment could wear off over time. Once the entire drainage area has been treated with the laser, further treatments may be ineffective. Conventional surgery for eye disease, also called filtering microsurgery, creates a new opening for the intraocular fluid to leave the eye. It typically is suggested when medications and/or optical device surgery have did not management pressure level. The surgery involves removing atiny low piece of the white, outer shell of the eye to create a channel through which the aqueous humor fluid can flow. This incisional surgery has been between 60 percent and 80 percent effective in lowering pressure.
- What can I do to prevent glaucoma?There is no known way to prevent glaucoma. However, vision loss from glaucoma can be prevented if the disease is detected and treated in time. Because glaucoma rarely produces symptoms until it has progressed, regular eye examinations are the key to early detection and treatment. For those with no risk factors, the American Academy of Ophthalmology recommends a complete eye exam once in your 20s and twice in your 30s. You should have a baseline comprehensive eye exam at age 40, and your eye doctor will recommend follow-up exams based on your family history and the results of the baseline exam. After age 65, it’s important to have a complete eye exam every year or two. take special vitamin supplements. What should I be taking and in what dose?Although glaucoma can’t be prevented, maintaining a healthy lifestyle and eating nutritious foods may help you generally avoid diseases. Eating a balanced diet is the best way to ensure your body receives the proper nutrients it needs to function. Some of the vitamins and minerals that will contribute to overall eye health embody inhibitor vitamins A, C and E, and minerals zinc, copper and selenium. If you’re concerned about your diet, talk with your health care professional about whether you should take nutritional supplements or make dietary changes.
- Can exercise help my glaucoma?Getting regular exercise also is a component of maintaining good overall health, and there is some evidence in the medical literature that regular aerobic exercise may help reduce eye pressure. Before starting any exercise program, make sure you discuss possible effects on your intraocular pressure with your health care professional. Some forms of glaucoma, such as angle-closure, are unresponsive to exercise or run the risk of increasing eye pressure. Exercise can increase the pressure in pigmentary glaucoma. Additionally, exercises or yoga movements that hold the head upside down have the potential for increasing eye pressure and generally are discouraged for everyone with glaucoma. Talk with your health care professional about what kind of exercise is best for you.
- Is there any special way I should take my glaucoma eye drops?The most important thing to remember when taking glaucoma medications is to take them exactly as directed by your health care professional. Make sure you understand how and when to take your medications and how to properly store them. For the medication to figure effectively, they need to be taken frequently and while not interruption. You will need to take them as long as they control your eye pressure.


